Spaced retrieval practice may be the magic spell you are looking for. An immune role for platelets.
Why a podcast?!
In this premier episode of The A&P Professor podcast (TAPP Radio), host Kevin Patton introduces himself and his reasons for launching this new series. (0:49)
Platelets as potent scavengers of bacteria? Really?
Something like 750 billion tiny cell fragments called platelets circulate in the human blood stream. When an injury to a blood vessel occurs, they stick to the exposed collagen in groups—forming platelet plug. And trigger additional reactions that eventually result in a blood clot.
But did you know that they have other helpful jobs, too? Like rounding up bacteria and feeding them up to immune cells, which devour them to make us safe.
This innate immune function of platelets has recently been outlined by researchers, as the information below summarizes.
Read through the quick points below to get an overview of some immune functions of platelets. Then read the full articles if you want to know more about these discoveries—including some great diagrams, micrographs, and videos.
Quick points about platelets as bacterial scavengers
At sites of vessel injury/inflammation, platelets that contact intact collagen stick together—but platelets that do not contact collagen are motile.
Motile platelets change shape from a "fried egg" to a polarized "half moon" to better navigate the shearing forces of blood flow.
They can even navigate "upstream" against the flow of blood.
Platelets can use mechanical force to pull particles—including bacteria—from surrounding substrates.
Platelets collect and bundle bacteria, which facilitates neutrophil activation and subsequent phagocytosis.
Migration pattern of motile platelet (left). Platelets collecting bacteria into bundles.
What can we use from this in teaching undergraduate A&P?
Yeah, okay we don't have time to go into all the ins and outs of platelets in a typical A&P course, but we canmention that platelets are now known to have immune functions.
Consider circling back to this mention later, when (if) you cover innate immune mechanisms a bit later in the course.
Consider calling attention to the sensory functions needed for platelets to analyze their microenvironment within the bloodstream.
Consider pointing out the specialized structure and function of the platelet's plasma membrane.
Integrins (integral membrane proteins) have a role in detecting particles for adhesion, binding to them, and sorting them.
Invaginations of the plasma membrane facilitate bundling of bacteria.
The shape changes needed for migration and handling of bacteria require actin-myosin reactions to power them. As in muscle fibers, these contractions are triggered by influx of extracellular calcium. In case you want to circle back to that.
Perhaps we should make a stronger point in reminding students that although they are "cell fragments" without a nucleus, they're more than just bags of hemostatic chemicals.
All these opportunities to "circle back" to previously studied concepts helps students make connections in their developing conceptual framework. And help them form a better understanding of the "big picture."
Introduction to the Gaertner, et. al., paper below—giving background and overview to enhance understanding of the new discoveries. Great diagram, too! Click "Supplemental information" in the article to access video clips.
Journal article describing the scavenger role of platelets. Includes a few very nice, simple diagrams—and some cool micrographs and data graphs. These can also be downloaded as PowerPoint slides. Click "Supplemental information" in the article to access video clips.
[NOTE: If you can't access the full text of any resource, ask your school's reference librarian for help. If they can't provide direct access, they'll probably know how to get a copy of the resource for you. Quickly.]
So why, exactly, is it that we should consume a lot of fiber in our diet to remain healthy? Are refined fiber supplements just as good as, say, an "apple a day?"
Recently, an article in the journal Cell answer seems to verify some of the answers for us.
As the paper cited below indicates, research seems to confirm that dietary fiber provides nutrients for the inhabitants of our intestinal microbiome. When dietary fiber is missing, then the microbes undergo a shift in populations and start consuming our GI mucus as an alternate source of nutrition. That, as you might guess, reduces the thickness of the protective mucus—hus increasing the likelihood that pathogens can more easily attack the intestinal lining. Ouch.
Apparently, refined prebiotic fibers don't fix the problem.
Here are some highlights of the research article (quoted from their online preview):
Characterized synthetic bacterial communities enable functional insights in vivo
Low-fiber diet promotes expansion and activity of colonic mucus-degrading bacteria
Purified prebiotic fibers do not alleviate degradation of the mucus layer
Fiber-deprived gut microbiota promotes aggressive colitis by an enteric pathogen
What can we use from this in teaching undergraduate A&P?
When asked by students about dietary fiber, you have more information from which to draw an answer.
When discussing any of these topics, you'll now have a bit more to add to your story:
nutrition
function of mucus
the human microbial system (or specifically, the GI microbiome)
how pathogens cause disease (or specifically, GI disorders)
Want to know more?
Veggies and Intact Grains a Day Keep the Pathogens Away
Francesca S. Gazzaniga. Dennis L. Kasper. Cell. Available online 17 November 2016
Brief preview of the M. Desai article cited below.
Every once in a while, I get an A&P student who expresses the concept of a negative Rh blood type as "having negative blood"—along with the connotation that having this blood type has a negative health impact.
We do not ordinarily think about red blood cell types such as A, B, AB, O, Rh+/-, or others, as being "bad for you" or even "good for you" healthwise. We most often think of them simply as different "flavors" of RBCs present in the human population.
Oh yeah, there are specific situations in which have a particular blood type can have significant health consequences. If you need an organ or tissue transplant—especially a blood donation—having the same RBC type as the available donor supply is "good for you." The lack thereof, then, is "bad for you" to at least some degree. Just like being tall can be bad for you when going through a low doorway.
Likewise, we all know there are health risks associated with a Rh- mother carrying an Rh+ fetus—especially the situation is not identified or if precautions are not taken. But it's not like the Rh- type itself has a direct health impact on the person with that type.
However, such a view may be a bit more complex than it first seems. Research continues to confirm that having a particular RBC type may affect your risk for certain health conditions.
For example, a little over a year ago, research published in the journal Neurology found that adults with type AB blood were at an increased risk of cognitive impairment compared to type O. Of course, much more work needs to be done to establish a potential mechanism for this phenomenon. But it does give some evidence that the idea of certain blood types having health consequences may be true.
Other studies have suggested these links:
Type O may be linked to depression, anxiety, low (female) fertility
Type O and/or A may be linked to attention-deficit disorder (ADD) in children
Type B may be linked to a lower risk of ADD in children
Type A may be linked to obsessive-compulsive disorder and stomach cancer
Type A, B, and AB may be linked to heart disease and abnormal blood clotting
What can we use from this in teaching undergraduate A&P?
Another interesting aside to throw into an exploration of blood types to "liven up" the conversation a bit to motivate students.
Consider using a diagram of the actual ABO markers to show what's involved at the cellular level—and their similarity to each other.
One may want to mention that blood types may become a factor health professionals may look at when assessing health risks in patients
A classroom discussion on possible mechanisms of a blood-type—health risk could be interesting and useful. This could lead to some great insights about methods of scientific discovery. For example, what's the difference between correlation and cause? How confident should we be in one study?
Consider leading the discussion toward exactly what you want your students to know about blood types and health (e.g., blood donors and recipients, erythroblastosis fetalis, etc.)
Want to know more?
Blood Type Matters for Brain Health
A. Anderson and V. Stern. Scientific American MIND January 1, 2015
Brief article explains discovery that people with AB blood type are at higher risk for age-related cognitive decline. Also lists some of the other blood-type links I mentioned above.
The World Health Organization says it is likely that the virus will spread, as the mosquitoes that carry the virus are found in almost every country in the Americas.
Zika virus was discovered almost 70 years ago, but wasn’t associated with outbreaks until 2007. So how did this formerly obscure virus wind up causing so much trouble in Brazil and other nations in South America?
Where did Zika come from?
Zika virus was first detected in Zika Forest in Uganda in 1947 in a rhesus monkey, and again in 1948 in the mosquito Aedes africanus, which is the forest relative of Aedes aegypti. Aedes aegypti and Aedes albopictus can both spread Zika. Sexual transmission between people has also been reported.
Zika has a lot in common with dengue and chikungunya, another emergent virus. All three originated from West and central Africa and Southeast Asia, but have recently expanded their range to include much of the tropics and subtropics globally. And they are all spread by the same species of mosquitoes.
Until 2007 very few cases of Zika in humans were reported. Then an outbreak occurred on Yap Island of Micronesia, infecting approximately 75 percent of the population. Six years later, the virus appeared in French Polynesia, along with outbreaks of dengue and chikungunya viruses.
How did Zika get to the Americas?
Genetic analysis of the virus revealed that the strain in Brazil was most similar to one that had been circulating in the Pacific.
Brazil had been on alert for an introduction of a new virus following the 2014 FIFA World Cup, because the event concentrated people from all over the world. However, no Pacific island nation with Zika transmission had competed at this event, making it less likely to be the source.
There is another theory that Zika virus may have been introduced following an international canoe event held in Rio de Janeiro in August of 2014, which hosted competitors from various Pacific islands.
Another possible route of introduction was overland from Chile, since that country had detected a case of Zika disease in a returning traveler from Easter Island.
Most people with Zika don’t know they have it
According to research after the Yap Island outbreak, the vast majority of people (80 percent) infected with Zika virus will never know it – they do not develop any symptoms at all. A minority who do become ill tend to have fever, rash, joint pains, red eyes, headache and muscle pain lasting up to a week. And no deaths had been reported.
In early 2015, Brazilian public health officials sounded the alert that Zika virus had been detected in patients with fevers in northeast Brazil. Then there was a similar uptick in the number of cases of Guillain-Barré in Brazil and El Salvador. And in late 2015 in Brazil, cases of microcephaly started to emerge.
At present, the link between Zika virus infection and microcephaly isn’t confirmed, but the virus has been found in amniotic fluid and brain tissue of a handful of cases.
How Zika might affect the brain is unclear, but a study from the 1970s revealed that the virus could replicate in neurons of young mice, causing neuronal destruction. Recent genetic analyses suggest that strains of Zika virus may be undergoing mutations, possibly accounting for changes in virulence and its ability to infect mosquitoes or hosts.
The Swiss cheese model for system failure
The Swiss cheese model of accident causation. Davidmack via Wikimedia Commons, CC BY-SA
One way to understand how Zika spread is to use something called the Swiss cheese model. Imagine a stack of Swiss cheese slices. The holes in each slice are a weakness, and throughout the stack, these holes aren’t the same size or the same shape. Problems arise when the holes align.
With any disease outbreak, multiple factors are at play, and each may be necessary but not sufficient on its own to cause it. Applying this model to our mosquito-borne mystery makes it easier to see how many different factors, or layers, coincided to create the current Zika outbreak.
A hole through the layers
The first layer is a fertile environment for mosquitoes. That’s something my colleagues and I have studied in the Amazon rain forest. We found that deforestation followed by agriculture and regrowth of low-lying vegetation provided a much more suitable environment for the malaria mosquito carrier than pristine forest.
Increasing urbanization and poverty create a fertile environment for the mosquitoes that spread dengue by creating ample breeding sites. In addition, climate change may raise the temperature and/or humidity in areas that previously have been below the threshold required for the mosquitoes to thrive.
The second layer is the introduction of the mosquito vector. Aedes aegypti and Aedes albopictus have expanded their geographic range in the past few decades. Urbanization, changing climate, air travel and transportation, and waxing and waning control efforts that are at the mercy of economic and political factors have led to these mosquitoes spreading to new areas and coming back in areas where they had previously been eradicated.
A woman walks away from her apartment as health workers fumigate the Altos del Cerro neighborhood as part of preventive measures against the Zika virus and other mosquito-borne diseases in Soyapango, El Salvador January 21, 2016.
Jose Cabezas/Reuters
For instance, in Latin America, continental mosquito eradication campaigns in the 1950s and 1960s led by the Pan American Health Organization conducted to battle yellow fever dramatically shrunk the range of Aedes aegypti. Following this success, however, interest in maintaining these mosquito control programs waned, and between 1980 and the 2000s the mosquito had made a full comeback.
The third layer, susceptible hosts, is critical as well. For instance, chikungunya virus has a tendency to infect very large portions of a population when it first invades an area. But once it blows through a small island, the virus may vanish because there are very few susceptible hosts remaining.
Since Zika is new to the Americas, there is a large population of susceptible hosts who haven’t previously been exposed. In a large country, Brazil for instance, the virus can continue circulating without running out of susceptible hosts for a long time.
The fourth layer is the introduction of the virus. It can be very difficult to pinpoint exactly when a virus is introduced in a particular setting. However, studies have associated increasing air travel with the spread of certain viruses such as dengue.
When these multiple factors are in alignment, it creates the conditions needed for an outbreak to start.
Putting the layers together
My colleagues and I are studying the role of these “layers” as they relate to the outbreak of yet another mosquito-borne virus, Madariaga virus (formerly known as Central/South American eastern equine encephalitis virus), which has caused numerous cases of encephalitis in the Darien jungle region of Panama.
There, we are examining the association between deforestation, mosquito vector factors, and the susceptibility of migrants compared to indigenous people in the affected area.
In our highly interconnected world which is being subjected to massive ecological change, we can expect ongoing outbreaks of viruses originating in far-flung regions with names we can barely pronounce – yet.
Researchers recently demonstrated that a flu vaccine delivered using microneedles that dissolve in the skin can protect people against infection even better than the standard needle-delivered vaccine.
The new microneedle patch is made of dissolvable material, eliminating needle-related risks. Not to mention the sea change it may mean for patients with severe needle anxiety! I suspect this approach may also be more tolerable for many patients than oral and nasal vaccination methods. It is also easy to use without the need for trained medical personnel—making it ideal for use where healthcare resources are limited.
“Our novel transcutaneous vaccination using a dissolving microneedle patch is the only application vaccination system that is readily adaptable for widespread practical use,” said Professor Shinsaku Nakagawa, one of the authors of the study from Osaka University. “Because the new patch is so easy to use, we believe it will be particularly effective in supporting vaccination in developing countries.”
The new microneedle patch – MicroHyala – is dissolvable in water. The tiny needles are made of hyaluronic acid, a naturally occurring substance in tissue matrix and the synovial fluid that cushions the joints. When the patch is applied sort of like a Band-Aid, the needles pierce the epidermis of skin and dissolve into the body, taking the vaccine with them.
The researchers compared the new system to traditional needle delivery by vaccinating two groups of people against three strains of influenza: A/H1N1, A/H3N2 and B. None of the subjects had a bad reaction to the vaccine, showing that it is safe to use in humans. The patch was also effective: people given the vaccine using the microneedles had an immune reaction that was equal to or stronger than those given the vaccine by injection.
“We were excited to see that our new microneedle patch is just as effective as the needle-delivered flu vaccines, and in some cases even more effective,” said Professor Nakagawa.
Previous research has evaluated the use of microneedles made of silicon or metal, but they were not shown to be safe. Microneedles made from these materials also run the risk of breaking off in the skin, leaving tiny fragments behind. The new dissolvable patch eliminates this risk because the microneedles are designed to dissolve in the skin.
What can we use from this in teaching undergraduate A&P?
Consider mentioning this advance when discussing the layers of the skin, this giving a clinical application to pique student interest.
When discussing immunity and vaccination, consider mentioning this discovery.
If you discuss hyaluronic acid when covering histology, this information may help students realize the importance of knowing such details because of clinical applications of materials science.
Want to know more?
Clinical study and stability assessment of a novel transcutaneous influenza vaccination using a dissolving microneedle patch.
Existing dogma in neuroscience states that the brain does not possess the classical lymphatic drainage system found in other parts of body. However, a recent letter in the journal Nature reports the discovery of lymphatic vessels lining the dural sinuses in mice. These were shown to drain immune cells and cerebrospinal fluid (CSF) into the deep cervical lymph nodes.
Although more work is yet to be done in humans, this discovery will cause neuroscientists to revisit a number of concepts related to CSF and lymphatic drainage, as well as immune functions in the brain.
For example, do these new data truly challenge the notion of immune privilege in the nervous tissue of the central nervous system—or do they apply to the brain as an organ and allow for lymphatic drainage of tissues outside the nervous tissue of the brain?
What can we use from this in teaching undergraduate A&P?
When discussing CSF drainage, consider mentioning the possibility that filtration of CSF directly into dural sinuses may be augmented by the newly discovered lymphatic drainage.
If you discuss the dogma of the "immune privilege" of the brain, consider mentioning this possible challenge to the concept. This may trigger a great discussion of whether these newly discovered lymphatic vessels are truly "in the brain."
If you discuss disorders involving altered immunity, such as multiple sclerosis, consider mentioning this discovery.
Bringing up this new information may be useful in discussions related to the process of science—how existing concepts are sometimes challenged by new information, for example. Perhaps a discussion of the need for more investigation would stimulate students to think about what future steps can be taken to map out a possible lymphatic network in or around the brain.
Liven up your A&P class with a great video showing a gruesome attack by a killer T cell on a cancer cell. It's a fantastic bit of video microscopy produced by Cambridge University.
Okay, with the oddly soothing music score instead of a more appropriate score for the graphic violence shown in this video, it's not much of a horror flick. Especially when you consider that it's the "bad guy" cell getting whacked. But it is graphic and dramatic and impressive.
Just the thing to liven up a discussion of adaptive immunity, which (let's face it) can often cause a catatonic state in many students.
Looking for a supplemental hands-on activity with the immune system in your course?
Try the FREE online interactive Immunology Virtual Lab from the Howard Hughes Medical Institute.
It covers these concepts:
The basis of humoral immunity
The foundation for ELISA (enzyme-linked immunosorbent assay)
Potential errors in conducting an ELISA
Sensitivity and specificity of a diagnostic test
What can we use from this in teaching undergraduate A&P?
Link to this virtual lab activity from your online syllabus, course web page, or LMS (or in an email or tweet to students)
If you want to give course points for the lab, consider an online quiz or lab report submitted through your learning management system (LMS) or emailed to you.
Gives students a "real life" clinical lab application for the concepts they are learning in A&P.
Provides an immunology lab option for online/hybrid courses or wet labs that don't have funding for immunology experiments.
Want to know more?
Immunology Virtual Lab
BioInteractive. Howard Hughes Medical Institute. Accessed 16 Sep 2014.
This virtual lab teaches the procedures of performing an ELISA test to determine whether a particular antibody is present in a patient's blood sample.
It's that time of year, eh? Cold and flu season. And this week we have news from researchers giving us a bit more insight into the rhinoviruses that cause the common cold.
The unsurprising new discovery is that rhinoviruses replicate more efficiently—and therefore cause colds more effectively—in the nasal cavity than in the lungs because of a temperature difference. In mice, the animals used in the recent study, the immune mechanisms that fight off rhinoviruses work better in the warmer environment of the lung than in the cooler environment of the nasal cavity.
This phenomenon may be why a cold generally doesn't wreak the same havoc in lungs as do other respiratory viruses like influenza viruses. Rhinoviruses, as their name implies, generally remain limited to the nose.
What can we use from this in teaching undergraduate A&P?
When discussing the nasal cavity's vascularity and air-warming functions, we may want to point out that understanding the temperature gradient between the nose and lower respiratory tract has practical clinical applications. Such as why some pathogens are limited to the nose. And why cold weather may contribute to rhinvirus infection.
When discussing immunology, we may want to mention that body temperature—and sometimes organ temperature—can have an impact on how efficiently our immune mechanisms fight infection.
One could consider steering a conversation about "there is still no cure for the common cold" to a conversation about the fact that scientists are still working on understanding rhinoviruses—"and, oh, did you hear the latest .....?"
Want to know more?
Where Rhinovirus Replicates Best
Tracy Vence, The Scientist. Online. January 6, 2015.
Scientists reported today that adipocytes in mouse and human skin produce an antimicrobial peptide (AMP) called cathelicidin is response to Staph aureus infections, including MRSA. Experimental animals that were deficient in the AMP were more susceptible to skin infections.
Adipocytes may recognize S. aureus by detecting bacterial peptides with toll-like receptors (TLRs), but more work is needed to fully understand the mechanisms.
This finding adds more to our understanding of human skin as a vital part of our body's defenses against infection. It also opens the door to understanding how diabetes, metabolic syndrome, and other conditions can reduce resistance to skin infections by altering the availability of AMPs in the fat associated with skin.
All of this may eventually lead to additional—perhaps more effective—strategies in preventing or curing serious skin infections such as MRSA.
I realize that we generally think of fat cells as belonging to the hypodermis, not the dermis, as described in the research. However, recent evidence shows the presence of adipocytes in the dermis that are distinct from those in the hypodermis. These adipocytes derive from a common precursor cell that produces both dermal fibroblasts and intradermal adipocytes. These dermal adipocytes have been shown to have a role in wound healing and the regeneration of hair follicles. And the research summarized here suggests that they also have a role in immunity.
What can we use from this in teaching undergraduate A&P?
Mention this discovery when discussing the roles of adipose tissue and adipocytes in your coverage of tissues of the body.
Consider clarifying that dermal adipocytes are distinct from fat cells in the hypdermis. And perhaps mention that it's a detail often left out of introductory discussions of skin.
This is a good point to mention when discussing the protective functions of the skin when covering the integumentary system.
When discussing the immune system, this concept helps illustrate several important principles:
The role of the skin as the first line of defense against infection
The variety of mechanisms available in the skin to act defensively
The role of TLRs and pattern recognition in immunity
The fact that immunity is a role for many tissues—not just lymphocytes and other WBCs
Take a moment NOW to add this to your course notes!
Want to know more?
Killer Fat
J. Alcorn and J. Kolls. Science 2 January 2015: Science Vol. 347 no. 6217 pp. 26-27 DOI: 10.1126/science.aaa4567
Editorial summary of the research in plain English. Includes a really nice, simple illustration of the concept (includes FREE teaching slide)
Dermal adipocytes protect against invasive Staphylococcus aureus skin infection
L. Zhang1, et al. Science 2 January 2015: Vol. 347 no. 6217 pp. 67-71 DOI: 10.1126/science.126097
Original research article. Additional images available here, including some nice micrographs showing increase in adipocytes in response to S. aureus infection
I'll never forget when Ira Fritz, my doctoral committee chair, practically slapped a packet of artificial sweetener out of my hand as I was about to put it into my iced tea. "That stuff will kill you!" he said as he extracted from me an oath to swear off the stuff. I'm not sure I quite believed him, but to this day I still drink my iced tea unsweetened.
As usual, Ira was right. Recently another brick has been added to the foundation of his concern about sugar substitutes. Researchers have found that sweeteners such as saccharine, sucralose, aspartame can alter the microbial ecosystem of our gut in a way that promotes the development of glucose intolerance. Glucose intolerance is part of metabolic syndrome, one of the most significant epidemics of our (or any) era.
At least as interesting as this microbial mediation between our diet and our metabolic function is the fact that only those human subjects who were responders exhibited the changes observed. This underscores our emerging view about the individualized nature of human nutrition and metabolism.
What can we use from this in teaching undergraduate A&P?
We have yet another example to share regarding why and how the human microbial system plays such a vital role in our body.
This may be an interesting story to bring up when discussing immunity in our A&P course, perhaps giving a preview of later topics on the gut microbiome and nutrition/metabolism.
Nutrition and metabolism are not the same for everyone. So the basic principles learned in an A&P course are likely to be generally true for humans, but not necessarily entirely true for every individual.
Yet another example of the principle "you are what you eat."
And here's another case of continued scientific research refining the story of what we know about human structure and function. Consider mentioning it when you are explaining scientific methodology and it's relevance to A&P at the start of your course. An interesting discussion may ensue after asking, "does this mean we should stop using sugar substitutes?"
Want to know more?
Artificial Sweeteners Linked to Glucose Intolerance
Beth Skwarecki.Medscape Medical News. September 17, 2014
Sugar Substitutes, Gut Bacteria, and Glucose Intolerance
Anna Azvolinsky. TheScientist. September 17, 2014
Another plain-English article covering how the consumption of artificial sweeteners results in glucose intolerance is mediated by changes in the gut microbiota in both mice and humans.
Consumption of artificially and sugar-sweetened beverages and incident type 2 diabetes in the Etude Epidémiologique auprès des femmes de la Mutuelle Générale de l'Education Nationale–European Prospective Investigation into Cancer and Nutrition cohort
Guy Fagherazzi, et al. American Journal of Clinical Nutrition. January 30, 2013.
Original research article about the diet soda-diabetes link.
A recent article in The Scientist once again reminds us of the ongoing explosion in the scientific understanding of the human microbial system. In a few short years, this area of exploration has moved to the forefront of medical and basic science research in human biology.
I think it's becoming clear that the most useful way to think of human body function is to recognize that an "organism" is really a sort of "habitat." And like any habitat, it functions best when all the inhabitants are within a limited range of balanced relationships.
Who are the inhabitants? Besides our own cells? Well, one could think of mitochondria and cilia and other organelles as symbiotic internal inhabitants of our cells. They're not that literally, of course, but I think its a useful metaphor for understanding the human body. Then there are the many microbes and animals that cover our internal and external surfaces, burrow into some of our pores and glands, and inhabit our body fluids.
I call the balanced functional relationship among the various microbomes of the body and our own tissues the human microbial system. And I am certain that it won't be long before we will be discussing this system alongside the major organ systems of the body. That is if we truly want to understand how the body really works.
The article in The Scientist I mention is a great summary of some of the major roles that the human microbial system plays in the human body—and a good survey of some of the areas of the body where the human-microbial functional relationships play out. See the link to the article below.
What can we use from this in teaching undergraduate A&P?
Why not introduce the concept of the human microbial system at the beginning of our A&P course, when we set the stage by explain how scientists understand the body and its functions as an integrated system of different parts?
We can mention the different microbiomes of the body when we explore each organ system where they play an important role—which is pretty much all of them!
Consider discussing what happens to normal human function when microbiomes get out of balance. For example, in the gut a microbial imbalance can lead to ulcers, diarrhea, and other dysfunctions. On the skin a pathogenic microbe may become dominant and cause a rash.
Promote a discussion of what kinds of wellness strategies might be employed to prevent microbial imbalances.
Our students can leave our A&P course with an up-to-date understanding of human biology that will help them understand new clinical concepts and treatment strategies.
Want to Know More?
The Body’s Ecosystem
By The Scientist Staff. The Scientist. August 1, 2014
Plain-English article (cited above) on how research on the human microbiome is booming, and scientists have moved from simply taking stock of gut flora to understanding the influence of microbes throughout the body.
Radio stories from National Public Radio on human microbiomes and their role in health and disease. The growing number of these stories tells us something as A&P teachers: maybe we better be covering this!
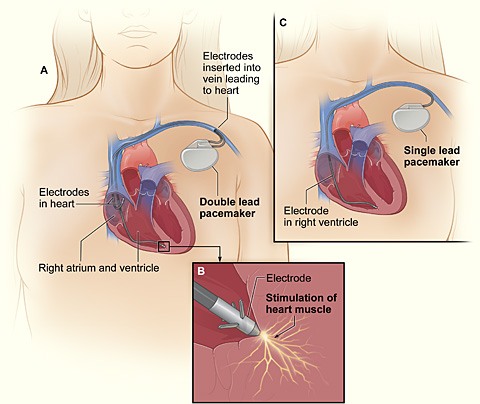
Researchers recently induced ordinary cardiac muscle fibers into becoming functioning pacemaker cells by injecting a therapeutic gene.
Working with pigs, a common model for human cardiovascular research, researchers first destroyed the natural pacemaker cells in each subject's heart and installed an electronic pacemaker. They then inserted a gene for transcription factor TBX18 into cardiac muscle tissue using an adenovirus. Using adenovirous vectors for inserting genes is a common strategy in gene therapy.
Within a couple of days, ordinary myocardial fibers had developed the structure and function of pacemaker cells. In about 5 days, the electronic pacemakers were no longer needed.
However, this biological pacemaking peaked at about 8 days, then eventually disappeared. This may occur because the virus-infected cells are probably destroyed by the body's immune defenses. So researchers are thinking that perhaps, at the very least, this could eventually lead to a temporary treatment for certain arrythmias in humans.
What can we use from this in teaching undergraduate A&P?
This is an interesting bit of news that helps illustrate the frontiers of human biomedical sciences.
This story provides a good case to provoke a discussion of the nature of gene therapy.
Why did the effect last only 8 or so day?
What does this tell us about transcription factor TBX18?
What benefit might this treatment have if developed for humans?
This may add interest to an discussion of the function of the electrical system of the heart in general, and artificial pacemakers in particular.
The case also provides a scenario in which the body attacks and destroys virus-infected cells.
Yesterday, the scientific community lost a true pioneer . . . Joseph Murray, who pioneered skin grafting and developed the first successful organ transplant. In 1954, he transplanted a kidney from one adult twin to his identical sibling. He continued to pioneer transplant techniques that have saved countless lives.
"In the twentieth century, Joseph Murray . . . noticed that skin he grafted onto burned soldiers he treated during World War II would eventually be rejected by the body. After the war, Murray tried to understand the body’s immune reactions to transplanted tissues and his work led to the first successful kidney transplants. His breakthroughs in transplanting kidneys not only earned him a Nobel Prize in 1990, it also paved the way for all the different types of tissue and organ transplantation that we see today."
93-year-old Joseph E. Murray suffered a stroke on Thanksgiving day and died yesterday in Boston.
I think the occasional story of a pioneer in the history of human science adds a lot to the A&P course. Such stories give a human dimension to the pursuit of science and provide the context needed for students to understand how we know what we know.
Today we have a sad but important occasion to bring up the amazing accomplishments of Joseph E. Murray with our students.
Want to know more?
Joseph E. Murray, Transplant Doctor and Nobel Prize Winner, Dies at 93
By CORNELIA DEAN
The New York Times Published online: November 27, 2012
Hope, Innovation: Remembering A Transplant Pioneer
Renee Montagne
National Public Radio (NPR) Morning Edition Broadcast/published online November 27, 2012
[Renee Montagne talks with Dr. Atul Gawande about the life and work of Dr. Joseph E. Murray, who performed the first successful organ transplant in 1954. Murray died Monday at age 93.]
Nobel Web (nobelprize.org) Accessed 27 November 2012
[Interview with Joseph E. Murray by Sten Orrenius at the meeting of Nobel Laureates in Lindau, Germany, June 2000. Joseph Murray talks about what led him into research; developing transplantation medicine (2:38); and whether breakthroughs in clinical research are often ignored by the Nobel Prize Committee (13:10).]
Nobel Web (nobelprize.org) Accessed 27 November 2012
[Joseph E. Murray held his Nobel Lecture on 8 December 1990, at Karolinska Institutet, Stockholm. He was presented by Professor Hans Wigzell of the Karolinska Institutet.]
for their discoveries concerning the activation of innate immunity
and the other half to
Ralph M. Steinman
for his discovery of the dendritic cell and its role in adaptive immunity
Summary
This year's Nobel Laureates have revolutionized our understanding of the immune system by discovering key principles for its activation.
Scientists have long been searching for the gatekeepers of the immune response by which man and other animals defend themselves against attack by bacteria and other microorganisms. Bruce Beutler and Jules Hoffmann discovered receptor proteins that can recognize such microorganisms and activate innate immunity, the first step in the body's immune response. Ralph Steinman discovered the dendritic cells of the immune system and their unique capacity to activate and regulate adaptive immunity, the later stage of the immune response during which microorganisms are cleared from the body.
The discoveries of the three Nobel Laureates have revealed how the innate and adaptive phases of the immune response are activated and thereby provided novel insights into disease mechanisms. Their work has opened up new avenues for the development of prevention and therapy against infections, cancer, and inflammatory diseases.
Two lines of defense in the immune system
We live in a dangerous world. Pathogenic microorganisms (bacteria, virus, fungi, and parasites) threaten us continuously but we are equipped with powerful defense mechanisms (please see image below). The first line of defense, innate immunity, can destroy invading microorganisms and trigger inflammation that contributes to blocking their assault. If microorganisms break through this defense line, adaptive immunity is called into action. With its T and B cells, it produces antibodies and killer cells that destroy infected cells. After successfully combating the infectious assault, our adaptive immune system maintains an immunologic memory that allows a more rapid and powerful mobilization of defense forces next time the same microorganism attacks. These two defense lines of the immune system provide good protection against infections but they also pose a risk. If the activation threshold is too low, or if endogenous molecules can activate the system, inflammatory disease may follow.
The components of the immune system have been identified step by step during the 20th century. Thanks to a series of discoveries awarded the Nobel Prize, we know, for instance, how antibodies are constructed and how T cells recognize foreign substances. However, until the work of Beutler, Hoffmann and Steinman, the mechanisms triggering the activation of innate immunity and mediating the communication between innate and adaptive immunity remained enigmatic.
Discovering the sensors of innate immunity
Jules Hoffmann made his pioneering discovery in 1996, when he and his co-workers investigated how fruit flies combat infections. They had access to flies with mutations in several different genes including Toll, a gene previously found to be involved in embryonal development by Christiane Nüsslein-Volhard (Nobel Prize 1995). When Hoffmann infected his fruit flies with bacteria or fungi, he discovered that Toll mutants died because they could not mount an effective defense. He was also able to conclude that the product of the Toll gene was involved in sensing pathogenic microorganisms and Toll activation was needed for successful defense against them. Bruce Beutler was searching for a receptor that could bind the bacterial product, lipopolysaccharide (LPS), which can cause septic shock, a life threatening condition that involves overstimulation of the immune system. In 1998, Beutler and his colleagues discovered that mice resistant to LPS had a mutation in a gene that was quite similar to the Toll gene of the fruit fly. This Toll-like receptor (TLR) turned out to be the elusive LPS receptor. When it binds LPS, signals are activated that cause inflammation and, when LPS doses are excessive, septic shock. These findings showed that mammals and fruit flies use similar molecules to activate innate immunity when encountering pathogenic microorganisms. The sensors of innate immunity had finally been discovered.
The discoveries of Hoffmann and Beutler triggered an explosion of research in innate immunity. Around a dozen different TLRs have now been identified in humans and mice. Each one of them recognizes certain types of molecules common in microorganisms. Individuals with certain mutations in these receptors carry an increased risk of infections while other genetic variants of TLR are associated with an increased risk for chronic inflammatory diseases.
A new cell type that controls adaptive immunity
Ralph Steinman discovered, in 1973, a new cell type that he called the dendritic cell. He speculated that it could be important in the immune system and went on to test whether dendritic cells could activate T cells, a cell type that has a key role in adaptive immunity and develops an immunologic memory against many different substances. In cell culture experiments, he showed that the presence of dendritic cells resulted in vivid responses of T cells to such substances. These findings were initially met with skepticism but subsequent work by Steinman demonstrated that dendritic cells have a unique capacity to activate T cells.
Further studies by Steinman and other scientists went on to address the question of how the adaptive immune system decides whether or not it should be activated when encountering various substances. Signals arising from the innate immune response and sensed by dendritic cells were shown to control T cell activation. This makes it possible for the immune system to react towards pathogenic microorganisms while avoiding an attack on the body's own endogenous molecules.
From fundamental research to medical use
The discoveries that are awarded the 2011 Nobel Prize have provided novel insights into the activation and regulation of our immune system. They have made possible the development of new methods for preventing and treating disease, for instance with improved vaccines against infections and in attempts to stimulate the immune system to attack tumors. These discoveries also help us understand why the immune system can attack our own tissues, thus providing clues for novel treatment of inflammatory diseases.
Bruce A. Beutler was born in 1957 in Chicago, USA. He received his MD from the University of Chicago in 1981 and worked as a scientist at Rockefeller University in New York and the University of Texas in Dallas, where he discovered the LPS receptor. Since 2000 he has been professor of genetics and immunology at The Scripps Research Institute, La Jolla, USA. Jules A. Hoffmann was born in Echternach, Luxembourg in 1941. He studied at the University of Strasbourg in France, where he obtained his PhD in 1969. After postdoctoral training at the University of Marburg, Germany, he returned to Strasbourg, where he headed a research laboratory from 1974 to 2009. He has also served as director of the Institute for Molecular Cell Biology in Strasbourg and during 2007-2008 as President of the French National Academy of Sciences. Ralph M. Steinman was born in 1943 in Montreal, Canada, where he studied biology and chemistry at McGill University. After studying medicine at Harvard Medical School in Boston, MA, USA, he received his MD in 1968. He has been affiliated with Rockefeller University in New York since 1970, has been professor of immunology at this institution since 1988, and is also director of its Center for Immunology and Immune Diseases.
Key publications:
Poltorak A, He X, Smirnova I, Liu MY, Van Huffel C, Du X, Birdwell D, Alejos E, Silva M, Galanos C, Freudenberg M, Ricciardi-Castagnoli P, Layton B, Beutler B. Defective LPS signaling in C3H/HeJ and C57BL/10ScCr mice: Mutations in Tlr4 gene. Science 1998;282:2085-2088.
Lemaitre B, Nicolas E, Michaut L, Reichhart JM, Hoffmann JA. The dorsoventral regulatory gene cassette spätzle/Toll/cactus controls the potent antifungal response in drosophila adults. Cell 1996;86:973-983.
Steinman RM, Cohn ZA. Identification of a novel cell type in peripheral lymphoid organs of mice. J Exp Med 1973;137:1142-1162.
Steinman RM, Witmer MD. Lymphoid dendritic cells are potent stimulators of the primary mixed leukocyte reaction in mice. Proc Natl Acad Sci USA 1978;75:5132-5136.
Schuler G, Steinman RM. Murine epidermal Langerhans cells mature into potent immunostimulatory dendritic cells in vitro. J Exp Med 1985;161:526-546.
The Nobel Assembly, consisting of 50 professors at Karolinska Institutet, awards the Nobel Prize in Physiology or Medicine. Its Nobel Committee evaluates the nominations. Since 1901 the Nobel Prize has been awarded to scientists who have made the most important discoveries for the benefit of mankind.
Nobel Prize® is the registered trademark of the Nobel Foundation
The information above is taken directly from
The 2011 Nobel Prize in Physiology or Medicine - Press Release
Nobelprize.org. 3 Oct 2011 my-ap.us/pE7zzC
Want to know more?
Immune Responses
[An animated activity from the Nobel Prize folks.]
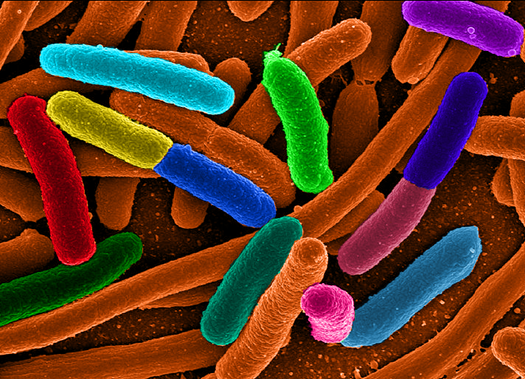
Remember my previous post, in which I gave you a free slide show on the role of the appendix in keeping the gut microbiome happy? Well, to sort of "prove the point" of the importance of a healthy gut microbiome, we've been hearing all about that weird Escherichia coli (E. coli) epidemic in Europe.
If you're like me, you'll want to take the opportunity to emphasize concepts learned in class by applying them to "real life" events reported in the news. If you're like me, you may want to check out these journal articles:
Deadly bugs: Toxin-producing E. coli strain causes outbreak in Germany Tina Hesman Saey Science News web edition : Tuesday, June 7th, 2011 my-ap.us/lfMeYE
[Brief, highly readable introduction to the current outbreak in Europe. Plus a cool photo!]
Bacterial infections: new and emerging enteric pathogens
Sherman, P et al. Current Opinion in Gastroenterology:January 2010 - Volume 26 - Issue 1 - p 1-4
doi: 10.1097/MOG.0b013e328333d73b my-ap.us/lJv8PC
[from the abstract: "The aim of this review is to highlight recent advances in knowledge of bacterial enteric infections. We focus on understanding of enterohemorrhagic Escherichia coli O157:H7 and Campylobacter jejuni infections, and to link these acute events with long-term consequences in a susceptible host, including irritable bowel syndrome and chronic inflammatory bowel diseases."]
Clinical Relevance of Shiga Toxin Concentrations in the Blood of Patients With Hemolytic Uremic Syndrome Brigotti, Maurizio et al. Pediatric Infectious Disease Journal: June 2011 - Volume 30 - Issue 6 - pp 486-490
doi: 10.1097/INF.0b013e3182074d22 my-ap.us/j72bUA [from the abstract: "Intestinal infections with Shiga toxin-producing Escherichia coli (STEC) in children can lead to the hemolytic uremic syndrome (HUS). Shiga toxins (Stx) released in the gut by bacteria enter the blood stream and target the kidney causing endothelial injury. Free toxins have never been detected in the blood of HUS patients, but they have been found on the surface of polymorphonuclear leukocytes (PMN)."]
Infectious colitis Navaneethan, Udayakumar and Giannella, Ralph A Current Opinion in Gastroenterology: January 2011 - Volume 27 - Issue 1 - p 66–71
doi: 10.1097/MOG.0b013e3283400755 my-ap.us/mTOlpN [from the abstract: "The incidence of gastrointestinal infections continues to increase and infectious colitis contributes to significant morbidity and mortality worldwide. The purpose of this review is to highlight the recent advances in knowledge of pathogens causing infectious colitis. We describe the various pathogens and specifically focus on enterohemorrhagic Escherichia coli (EHEC) O157:H7, Salmonella, Shigella, Campylobacter, and Entamoeba histolytica infections, and their impact on long-term effects, including postinfectious irritable bowel syndrome and inflammatory bowel disease."]
An inside job: subversion of the host secretory pathway by intestinal pathogens Sharp, Tyler M and Estes, Mary K Current Opinion in Infectious Diseases: October 2010 - Volume 23 - Issue 5 - p 464–469
doi: 10.1097/QCO.0b013e32833dcebd my-ap.us/leb7Le [from the abstract: "The cellular secretory pathway, composed of the endoplasmic reticulum, Golgi apparatus, and cellular vesicles, mediates the intracellular trafficking of proteins and lipids. Gastrointestinal pathogens frequently affect the functions of enterocytes, the differentiated cells involved in secretion and absorption of extracellular molecules. Microbial pathogenesis can be enhanced by altering the trafficking of key molecules such as brush border enzymes, soluble immune mediators such as cytokines and chemokines, and MHC Class I molecules, all of which rely on the secretory pathway for their appropriate cellular localization. This review focuses on our current understanding of the distinct mechanisms employed by enteric pathogens to antagonize the secretory pathway."]
Probiotics: progress toward novel therapies for intestinal diseases Yan et al. Current Opinion in Gastroenterology: March 2010 - Volume 26 - Issue 2 - p 95–101
doi: 10.1097/MOG.0b013e328335239a my-ap.us/iH93qP [from the abstract "As the beneficial effects of probiotics on health and disease prevention and treatment have been well recognized, the demand for probiotics in clinical applications and as functional foods has significantly increased in spite of limited understanding of the mechanisms. This review focuses on the most recent advances in probiotic research from genetics to biological consequences regulated by probiotics and probiotic-derived factors."]
For a really cool, copyright-free image to use in your course, go to my-ap.us/lVEg69


























{kind=link}
{kind=link}